
Maternal Mortality
South Dakota's Maternal Mortality in the Last Decade
What are pregnancy-associated deaths?
Pregnancy-associated deaths happen during pregnancy or within a year after it ends. Understanding these tragedies helps us improve care and prevent future losses.
A Decade of Data (2015-2024)
Over the last 10 years, 75 South Dakota mothers lost their lives during or shortly after pregnancy. This represents an average mortality rate of 65.7 deaths per 100,000 live births, based on 116,110 total births.
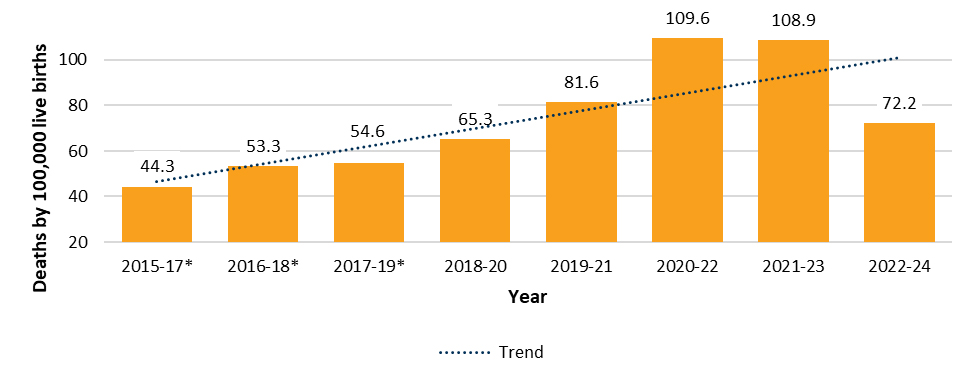
Source: Birth and Death records. Office of Health Statistics, Department of Health.
*Rates are unreliable due to small numbers of cases and should be considered with caution.
Disparities That Cannot Be Ignored
The data also reveals troubling gaps. Mothers from certain racial and ethnic groups faced much higher risks. For example, the mortality rate for American Indian/Alaskan Natives reached 188.0 deaths per 100,000 live births, compared to just 35.7 deaths per 100,000 for White moms.

Source: Birth and Death records. Office of Health Statistics, Department of Health.
Note: Rates for all other race and ethnicity groups were excluded due to small numbers of cases that made rates extremely unreliable.
Maternal Age Matters
Young mothers face greater risks. Mothers under 20 years old experienced the highest mortality rate of 141.5 deaths per 100,000 live births. In comparison, mothers aged 20–29 had a rate of 58.1 deaths per 100,000, and those aged 30–39 had a rate of 63.3 deaths per 100,000.

*Rate is unreliable due to the small number of cases and should be considered with caution.
**Suppressed due to very small numbers of cases that made the rate extremely unreliable.
Where You Live Can Make a Difference
Geographic disparities also play a role. The pregnancy-associated death rate in the Small Rural - Tribal group (148.1 per 100,000 live births) was three times higher than in the Rural - Non-Tribal group (48.6 per 100,000 live births).

*Rates are unreliable due to small numbers of cases and should be considered with caution.
Source: Birth and Death records. Office of Health Statistics, Department of Health.
Rural and tribal county classification: Office of Rural Health, Department of Health
Education and Outcomes
A mother’s education level can also impact outcomes. Those with a high school diploma or GED had the highest mortality rates (144.8 deaths per 100,000 live births), followed by mothers with less than a high school education (84.2 deaths per 100,000), both higher than the statewide 10-year rate. Rates were lowest among those with a bachelor’s degree (33.1 per 100,000).

*Rates are unreliable due to the small number of cases and should be considered with caution.
**Suppressed due to very small numbers of cases that made the rate extremely unreliable.
A Path Forward
South Dakota has the tools to address these challenges. Efforts are underway to:
- Improve access to high-quality prenatal, delivery, and postpartum care.
- Tackle social factors that contribute to health disparities.
- Provide education and resources to at-risk communities.
- Support healthcare providers with training and tools to manage complex pregnancies.
Maternal Mortality Reports
Pregnancy-Associated and Infant Deaths in South Dakota, 2015-2024
The following report describes the characteristics of mothers who died during pregnancy or within one year of the end of pregnancy, as well as infants who died before their first birthday, in South Dakota from 2015–2024. Throughout this report, we refer to these losses as pregnancy-associated deaths and infant deaths. There were 787 infant deaths during those 10 years, and 75 pregnancy-associated deaths.
South Dakota Maternal Mortality Review Committee
The South Dakota Department of Health's Maternal Mortality Review Committee (MMRC) is a multidisciplinary expert panel with representation from public health, nursing, maternal and fetal medicine, mental health, substance use, pathology, obstetrics/gynecology, and social work.
The South Dakota MMRC reviews all deaths of South Dakota residents that occur while pregnant or within one year of the end of pregnancy. The MMRC determines pregnancy-relatedness, preventability, and contributing factors to the death. The MMRC develops recommendations based on these factors to improve policies and practices and reduce preventable maternal deaths in South Dakota.
The South Dakota MMRC began reviewing cases in October 2021 and reviewed 20 cases in its first year. These deaths occurred from 2018-2021. SD MMRC committee members are listed below.
- Dr. Denise Hanisch, SD DOH, Chair
- Shelby Kommes, SD DOH, ERASE MM Project Officer
- Lori Koenecke, SD DOH/Black Hills Special Services, Case Abstractor
- Lorrie Lendvoy, SD DOH/Black Hills Special Services, Epidemiologist
- Leslie Krump, SD DOH, Nurse Manager- Bright Start Home Visiting
- Abhinav Datti, SD DOH, Prevention Services Manager
- Amanda Long-Stanley, Case Manager/Women's Advocate, Bethany Christian Services
- Dawn Nordquist, All Women Count Program Coordinator
- Dr. Mary Carpenter, Family Medicine MD
- Dr. Kimberly McKay, OBGYN, Avera McKennan Hospital and University Center
- Leah Stroschein, Detective, Lincoln County Sheriff's Office
- Dr. Maria Schmoll, Maternal & Fetal Medicine, Sanford Health
- Randee Peterson, Integrated Services Coordinator, Project Recovery
- Dr. Sarah Flynn, Psychiatrist, Sanford Health
- Tami Hogie-Lorenzen, CMO, SD Urban Indian Health